Reduction of pre-dinner anxiety in a group of adolescent patients with Anorexia Nervosa attending a Day Hospital treatment programme during lockdown due of COVID-19 in Italy: An observational study
Enrico Ceccato1,2 , Stefania Zanin1, Laura Merlino1, Chiara Bonetto2, Alessandra Sala1
1 Eating Disorder Unit, San Bortolo Hospital, Vicenza, Italy
2 Section of Psychiatry, Department of Neuroscience, Biomedicine and Movement Sciences, University of Verona, Verona, Italy
Abstract
Introduction: The COVID-19 pandemic and its associated restrictions have been linked to a general exacerbation of mental health symptoms, particularly within the spectrum of Eating Disorders (ED). While many studies report a worsening of symptoms, the specific impact on meal-related anxiety in clinical settings remains to be fully elucidated.
Aim: This study aims to describe the trajectory of pre-dinner anxiety in a small cohort of adolescent patients diagnosed with Anorexia Nervosa (AN) across three phases: before, during, and after the national lockdown in Italy.
Methods: A self-report tool, the "Thermometer of Discomfort," was used to assess anxiety levels in patients attending the Day Hospital (DH) treatment program at the Hospital of Vicenza between March 2020 and September 2020. Summary measures and percentage/rank changes were calculated for each patient across the three periods. Finally, a focus group was conducted to discuss the results with patients and gather their qualitative perspectives.
Results: 71.4% of patients reported a decrease in discomfort during the lockdown, while 57.1% experienced a subsequent increase in anxiety once the restrictions ended. During the focus group, almost all participants confirmed that their anxiety was lower during the lockdown period compared to the phases before or after.
Conclusion: Contrary to general trends, these patients showed a reduction in pre-dinner anxiety during the lockdown. The reduction in social exposure and the avoidance of external triggers may have acted as transitory protective factors. Furthermore, the continuation of Day Hospital care (continuity of care) likely played a crucial role in maintaining this stability.
Keywords
Eating Disorder
Covid-19
Anxiety
Lockdown
Anorexia Nervosa
Day Hospital
Introduction
The impact of the COVID-19 pandemic and its associated restrictive measures on individuals with Anorexia Nervosa (AN) has been predominantly negative (Branley-Bell et al., 2020; Monteleone, 2021a; Raffagnato et al., 2024).
Recent literature has confirmed that a decreased sense of control, social isolation, increased exposure to triggering media messages (Micanti et al., 2021), and heightened anxiety (Termorshuizen et al., 2020) fueled rumination on eating disorders and exacerbated psychological distress (Schlegl et al., 2020; Vuillier et al., 2021).
Longitudinal studies have highlighted that patients with Eating Disorders (ED) exhibited significantly higher levels of stress, depression, and PTSD-related symptoms compared to healthy controls (Monteleone et al., 2021b, Cecchetto et al., 2021), with these symptoms persisting well into the post-emergency phase (Devoe et al., 2023). During the lockdown, a concerning increase in compensatory exercise was observed (Castellini et al., 2020), often employed as a dysfunctional strategy to manage the loss of routine and physical distancing (Schlegl et al., 2020).
The worsening of general psychopathology was closely correlated with specific personality traits: low self-directedness and the adoption of maladaptive coping strategies were associated with greater symptom severity and weight fluctuations during lockdown (Baenas et al., 2020). Furthermore, difficulties in emotion regulation emerged as a critical factor (Leppanen et al., 2021), with recent evidence suggesting that emotional instability predicted treatment resistance even months after the lifting of restrictions (Monteleone et al., 2021c).
Although reduced access to specialist services presented monumental initial challenges (Linardon et al., 2022), current research has begun to explore the efficacy of continuity of care via telemedicine. Contrary to early observations, recent studies indicate that patients who continued treatment (including remote modalities) demonstrated greater resilience and symptomatic stability compared to those who experienced interruptions (Waller et al., 2020; Steiger et al., 2022). Notably, in the specific context of adolescents with Anorexia Nervosa, intensive Cognitive Behavioral Therapy (CBT-E) has proven to remain robust; recent data showed no significant differences in clinical outcomes (BMI and psychopathology) between patients treated before, during, and after the pandemic, suggesting that the efficacy of specialized care was not compromised by the restrictions or their aftermath (Dalle Grave et al., 2024). A multicenter study conducted in Italy emphasizes the crucial importance of maintaining a strong therapeutic alliance (even remotely) and supporting the patient’s social network, as these represent the true protective factors against worsening, more than the specific treatment techniques used (Monteleone et al., 2021c)
Finally, it remains noteworthy that for a minority of patients, the lockdown fostered positive effects, such as increased family support and more time dedicated to self-care (Termorshuizen et al., 2020).
Aim
The study aims to investigate fluctuations in self-perceived pre-dinner anxiety among a cohort of adolescent outpatients with Anorexia Nervosa (AN) attending a Day Hospital (DH) Treatment, during three distinct phases of the COVID-19 pandemic: pre-lockdown, during lockdown, and post-lockdown.
Methods
This observational study was conducted at the Day Hospital (DH) for Eating Disorders at the Hospital of Vicenza, Italy. Anxiety levels were monitored across three periods in 2020:
- T0 (Pre-lockdown): February 10 – March 4.
- T1 (Lockdown): March 10 – May 13.
- T2 (Post-lockdown): May 18 – September 16.
Notably, while most outpatient services in Italy were suspended by regional mandate on March 8, 2020, mental health services remained fully functional (D’Agostino et al., 2020). Consequently, patients were able to attend the DH treatment program through specific medical authorizations, ensuring continuity of care despite national restrictions. DH treatment program runs from Monday to Friday but dinner were only available on Monday, Tuesday and Wednesday.
In order to assess pre-dinner anxiety, we used a self-report Visual Analogue Scale (VAS) styled as a "Thermometer of Discomfort."
The task was: "Try to measure the level of your anxiety on a scale from 0 to 100" where 0 correspond to "completely relaxed" and 100 corresponds to "as much anxiety as possible". The scale ranges from 0 ("completely relaxed," indicated in green) to 100 ("maximum anxiety," indicated in red). Patients were instructed to rate their discomfort immediately before dinner on Mondays, Tuesdays, and Wednesdays (the days when meals are served within the DH program).
Data Analysis
The assessment was requested for a total of 8 days in T0, 21 days in T1, and 27 days in T2. Due to the explorative nature of the study and the very low sample size, no statistical test was applied. Descriptive measures (mean, standard deviation, median, and range) were calculated by using SPSS 26.
Clinical trajectories were analyzed through:
- Percentage variations in mean scores between T0-T1 and T1-T2. Changes (%) between the first two periods (t0 and t1) and the last two periods (t1 and t2) were calculated as (mean value t1 – mean value t0)/mean value t0*100 and (mean value t2 – mean value t1)/mean value t1*100, respectively.
- Rank analysis, categorizing scores into 10-point intervals (e.g., 0-10, 11-20) to track shifts in anxiety severity. In line with the pilot nature of the study, no inferential statistical tests were applied. The range 0-100 of the "Thermometer of discomfort" was divided in 10-width intervals such as 0-10, 11-20, 21-30, etc.) and the changes in ranking were explored for each patient.
Following the quantitative phase, a semi-structured unique session of 60 minutes focus group was conducted by the professional educator of the Day Hospital.
A rapid qualitative analysis procedure (RQAP) was utilized (Gale et al., 2019). The professional educator (SZ) developed a codebook based on the interview guide, which was iteratively updated during the coding process. The educator and the principal investigator reached consensus on the coding structure, organizing transcripts into summary tables including domains, categories, and illustrative quotes, representing the first step of the RQAP (Gale et al., 2019). The final tables were reviewed and validated by both to ensure consistency and analytic rigor. Findings were organized into a summary matrix structured by themes, following the second step of the RQAP.
The results were discussed with the patients and asked them what those results were due to. (Onwuegbuzie al., 2009).
The discussion was guided by three core questions (prepared as a guidance):
- Awareness of the rationale behind pre-dinner anxiety monitoring.
- Patients' predictions regarding the study's outcomes.
- Subjective explanations for the observed trends.
Responses were recorded and analyzed thematically by the principal investigator and the professional educator to provide a qualitative framework for the quantitative data.
Finally, the collected data were presented to and discussed with the patients.
Results
Of the 8 eligible patients, 7 (87.5%) were retained for the final analysis. One patient was excluded due to insufficient data (completion of less than 50% of the scheduled assessments in at least one study period). Table 1 reports the demographic and clinical characteristics of the sample.
Summary measures for the "Thermometer of Discomfort" at T0, T1, and T2 are detailed in Tables 2, 3, and 4.
Table 1. Demographic and Clinical Characteristics of the Sample
| Variable | Mean (± SD) |
| Number (total) | 7 |
| Gender, female (%) | 100 |
| Age (years) | 17.2 (± 2.5) |
| BMI at admission | 15.7 (± 1.9) |
| Age of Onset (years) | 14.7 (± 1.6) |
| Duration of Illness (years) | 2.5 (± 3.0) |
Note: BMI, Body Mass Index; SD, Standard Deviation.
Table 2. Pre-dinner perceived anxiety during pre-lockdown period (n=7)
| PRE-LOCKDOWN PERIOD (10 February 2020-4 March 2020) | ||||||
| Patient | Number of assessments | Mean | Standard deviation | Median | Minimum | Maximum |
| 1 | 8 | 58.7 | 31.2 | 70 | 15 | 90 |
| 2 | 8 | 79.4 | 10.2 | 80 | 60 | 90 |
| 3 | 8 | 53.7 | 31.9 | 50 | 10 | 90 |
| 4 | 8 | 71.9 | 22.7 | 80 | 20 | 90 |
| 5 | 8 | 62.5 | 30.0 | 72.5 | 20 | 90 |
| 6 | 8 | 60.6 | 27.3 | 55 | 20 | 100 |
| 7 | 8 | 60.6 | 34.0 | 62.5 | 15 | 100 |
Table 3. Pre-dinner perceived anxiety during lockdown period (n=7)
| LOCKDOWN PERIOD (10 March 2020-13 May 2020) | ||||||
| Patient | Number of assessments | Mean | Standard deviation | Median | Minimum | Maximum |
| 1 | 21 | 60.2 | 29.6 | 75 | 10 | 100 |
| 2 | 21 | 69.8 | 27.5 | 80 | 10 | 100 |
| 3 | 21 | 59.8 | 29.8 | 80 | 0 | 90 |
| 4 | 21 | 64.3 | 29.7 | 80 | 0 | 90 |
| 5 | 21 | 65.9 | 25.6 | 75 | 20 | 90 |
| 6 | 18 | 60.0 | 26.3 | 65 | 20 | 90 |
| 7 | 12 | 57.5 | 29.3 | 70 | 10 | 90 |
Table 4. Pre-dinner perceived anxiety during post-lockdown period (n=7)
| POST-LOCKDOWN PERIOD (18 May 2020-16 September 2020) | ||||||
| Patient | Number of assessments | Mean | Standard deviation | Median | Minimum | Maximum |
| 1 | 27 | 67.8 | 27.1 | 70 | 0 | 100 |
| 2 | 27 | 76.5 | 19.1 | 80 | 20 | 100 |
| 3 | 27 | 65.2 | 27.2 | 70 | 0 | 90 |
| 4 | 27 | 68.7 | 30.0 | 80 | 0 | 100 |
| 5 | 27 | 64.5 | 33.0 | 80 | 0 | 100 |
| 6 | 23 | 60.9 | 30.0 | 70 | 0 | 90 |
| 7 | 19 | 46.8 | 36.4 | 60 | 0 | 100 |
Quantitative Trends in pre-dinner Anxiety
Individual mean anxiety trajectories are illustrated in Figure 1. A heterogeneous response was observed:
- Decrease: Patients 2, 4, and 7 showed a downward trend in pre-dinner anxiety during the lockdown (T1), with Patient 7 maintaining this reduction into the post-lockdown period (T2).
- Stability: Patients 5 and 6 remained substantially stable throughout the study.
- Increase: Patients 1 and 3 exhibited a progressive increase in mean anxiety levels across all three periods.
The percentage variations in mean anxiety between periods are summarized in Table 5. Notably, a widespread increase in pre-dinner anxiety was observed following the cessation of lockdown measures (T2).
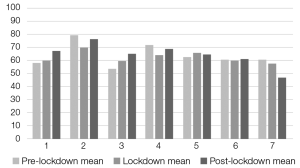
Figure 1. Pre-dinner perceived anxiety assessments (mean values) during the 3 periods (pre-lockdown, lockdown, post-lockdown) for each patient (n=7)
Rank Analysis
The categorical shift between anxiety "bands" (10-point intervals) is presented in Table 6. This analysis reveals that:
- T0 to T1: 5 patients (71.4%) transitioned to a lower anxiety rank during the lockdown, while 2 remained stable.
- T1 to T2: Upon the lifting of restrictions, 4 patients (57.1%) moved to a higher anxiety rank, 2 remained stable, and only 1 showed a further decrease.
Table 5. Pre-dinner perceived anxiety mean value changes (%) between the first two periods (pre-lockdown and lockdown) and the last two periods (lockdown and post-lockdown) for each patient (n=7)
|
PERIOD BETWEEN PRE-LOCKDOWN AND LOCKDOWN |
PERIOD BETWEEN LOCKDOWN AND POST-LOCKDOWN |
|||
| Patient | % changea | Pre-dinner anxiety trend | % changeb | Pre-dinner anxiety trend |
| 1 | +2.6 | Increased | +12.6 | Increased |
| 2 | -12.1 | Decreased | +9.6 | Increased |
| 3 | +11.4 | Increased | +9.0 | Increased |
| 4 | -10.6 | Decreased | +6.8 | Increased |
| 5 | +5.4 | Increased | -2.1 | Decreased |
| 6 | -1.0 | Decreased | +1.5 | Increased |
| 7 | -5.1 | Decreased | -18.6 | Decreased |
a % change calculated as: (lockdown mean value – pre-lockdown mean value)/pre-lockdown mean value*100
b % change calculated as: (post-lockdown mean value – lockdown mean value)/lockdown mean value*100
Table 6. Pre-dinner perceived anxiety ranking changes (the 0-100 range was divided in 10-width intervals 0-10, 11-20, 21-30, etc.) between the first two periods (pre-lockdown and lockdown) and the last two periods (lockdown and post-lockdown) for each patient (n=7)
| Patient | T0 Intervala | T1 Intervala | T2 Intervala | Rank change t0-t1 | Rank change t1-t2 |
| 1 | B | B | C | 0 | +1 |
| 2 | D | C | D | -1 | +1 |
| 3 | B | B | C | 0 | +1 |
| 4 | D | C | C | -1 | 0 |
| 5 | C | C | C | 0 | 0 |
| 6 | C | B | C | -1 | +1 |
| 7 | C | B | A | -1 | -1 |
a A: 41-50; B: 51-60; C: 61-70; D:71-80
Qualitative Findings: Focus Group
We briefly report, without going into detail, the outcomes of the focus group. The thematic analysis of the focus group revealed that while patients recognized the clinical importance of monitoring pre-dinner distress, they were unaware that the study aimed to track lockdown-specific fluctuations.
The majority of participants subjectively confirmed that their anxiety was lower during the lockdown period. Three primary themes emerged as potential reasons for this reduction:
- Social Environment and "Newness": Patients attributed higher anxiety levels after the lockdown to the admission of new peers to the DH. They noted that their own anxiety was highest upon admission and that the presence of new patients "reactivated" meal-related distress.
- Reduction of External Stimuli: There was a consensus that "normal life generates anxiety." The lockdown acted as a protective barrier against the overstimulation and social pressures of typical daily routines.
- The "Common Enemy" Phenomenon: Participants described a heightened sense of group cohesion and solidarity ("teaming up") against the external threat of the pandemic, which served as an emotional buffer.
Conversely, a minority of patients (one-third) reported a negative impact, citing boredom and the disruption of daily structure as factors that undermined their ability to regulate anxiety effectively.
Discussion
The results of our observational analysis, supported by qualitative focus group data, indicate a significant reduction in pre-dinner anxiety during the lockdown period.
Several patients reported a decrease in discomfort following the implementation of emergency measures and conversely, some patients reported a resurgence of anxiety once these restrictions were lifted.
Since the sample was analysed across three different periods during Day Hospital (DH) treatment, changes in pre-dinner anxiety levels across these periods may have been influenced by the treatment itself, which in general would be expected to reduce anxiety. We think it is crucial to highlight that this reduction in anxiety occurred within the context of continued Day Hospital (DH) care. Unlike many international cohorts that suffered from treatment interruption (Linardon et al., 2022), our patients maintained a structured clinical reference. Recent literature confirms that continuity of care, whether in-person via medical authorizations or through hybrid telemedicine, was the primary predictor of positive outcomes during the pandemic (Waller et al., 2020; Steiger et al., 2022).
Our findings suggest that the isolation imposed by the lockdown may have served as a temporary protective factor by physically removing patients from common interpersonal triggers. If social challenges and interpersonal hypersensitivity are core mechanisms in maintaining AN (Guerrini Usubini et al., 2021), the "pause" from social pressure likely provided symptomatic relief. Recent studies have termed this the "cocoon effect", where the reduction in social comparison and the "thin-ideal" pressure from the external environment led to a paradoxical stabilization in some adolescent patients (Graell et al., 2020; Schlegl et al., 2020). For these adolescents, the removal of stressful life events related to peer interactions—often cited as triggers for AN onset and relapse (Zipfel et al., 2022)—allowed for a focus on the self without external evaluative threat.
A compelling theoretical implication of our study relates to the concept of control. While over-control is a known maintenance factor for AN (Fairburn et al., 2003), the global scale of the COVID-19 pandemic highlighted the inherent uncontrollability of external events. Our results suggest that this collective "loss of control" may have fostered a greater capacity for radical acceptance. By recognizing that external factors (including the "worst-case" pandemic scenario) were beyond their influence, patients may have experienced a reduction in the maladaptive need to control their immediate environment, including meal-related distress. This is further supported by the "common enemy" sentiment expressed in the focus group, which enhanced group cohesion—a known therapeutic factor that may have buffered individual anxiety (Castellini et al., 2020).
Strengths and Limitations
A major strength of this study is its ecological validity; it was conducted in a real-world clinical setting without disrupting routine care. Furthermore, the blindness of the participants regarding the study's longitudinal comparative aim reduced social desirability bias. Lastly, we believe that the "Thermometer of Discomfort" reflected genuine self-perception, as it is a tool used routinely on a daily basis and patients are aware that it is employed by the clinical team in a supportive, non-judgmental manner.
However, several limitations must be acknowledged. The small sample size restricts the analysis to a descriptive and exploratory level, preventing the generalization of results. Additionally, the reliance on a single-item self-report tool ("discomfort") captures only a specific dimension of the patients' complex emotional state. Future research should investigate other potential moderators, such as family functioning or specific personality traits (e.g., self-directedness), which were not explored here. The Visual Analogue Scale (VAS) used, presented in the style of a "Thermometer of Discomfort," is not a formally validated instrument and was adopted as an exploratory measure of perceived discomfort. Its simplicity and visual immediacy may have facilitated participants’ understanding and use, allowing for an intuitive assessment of subjective experience. The results obtained with this scale should therefore be interpreted with caution and considered as indicative, pending further studies evaluating its reliability and validity.
Conclusions
In conclusion, our study suggests that for some adolescents with AN, the lockdown acted as a temporary "buffer" against environmental stressors, leading to reduced activation in front of the primary stressor: food. This "protective" effect, however, appears closely tied to the maintenance of intensive treatment services (DH). The increase in anxiety post-lockdown serves as a clinical reminder that while social avoidance may provide short-term relief, the resumption of "normal life" necessitates targeted support to manage the reactivation of social and meal-related distress.
What is already known on this subject?
The existing literature overwhelmingly indicates that the COVID-19 pandemic and its associated lockdowns had a detrimental impact on individuals with Eating Disorders. Most studies have reported a significant exacerbation of anxiety and depressive symptoms, which in turn led to an increase in the severity of disordered eating behaviors and a higher risk of relapse.
What does this study add?
Contrary to the prevailing narrative, this small observational study highlights a paradoxical trend: a reduction in self-perceived pre-dinner anxiety during the lockdown period. By integrating quantitative data with qualitative insights from a focus group, the study suggests that the reduction in social exposure and the "thin-ideal" pressure acted as a temporary protective "buffer." These findings emphasize the role of interpersonal stressors as key maintenance factors in adolescent Anorexia Nervosa and highlight the importance of continuity of care in intensive settings like Day Hospitals.
References
Baenas, I., Etuain, M., Fernández-Aranda, F., et al. (2021). Impact of COVID-19 lockdown on eating disorders: A multicentre collaborative study. Nutrients, 14(1), 100. https://doi.org/10.3390/nu14010100
Branley-Bell, D., & Talbot, C. V. (2020). Exploring the impact of the COVID-19 pandemic and UK lockdown on individuals with experience of eating disorders. Journal of Eating Disorders, 8, 44. https://doi.org/10.1186/s40337-020-00319-y
Castellini, G., Cassioli, E., Rossi, E., Innocenti, M., Gironi, V., Sanfilippo, G., Felciai, F., Monteleone, A. M., & Ricca, V. (2020). The impact of COVID-19 epidemic on eating disorders: A longitudinal observation of pre versus post psychopathological features in a sample of patients with eating disorders and a group of healthy controls. International Journal of Eating Disorders, 53(11), 1855–1862. https://doi.org/10.1002/eat.23368
Cecchetto, C., Aiello, M., Gentili, C., Ionta, S., & Osimo, S. A. (2021). Increased emotional eating during COVID-19 associated with lockdown, psychological and social distress. Appetite, 160, 105122. https://doi.org/10.1016/j.appet.2021.105122
D'Agostino, A., Demartini, B., Cavallotti, S., & Gambini, O. (2020). Mental health services in Italy during the COVID-19 outbreak. The lancet. Psychiatry, 7(5), 385–387. https://doi.org/10.1016/S2215-0366(20)30133-4
Dalle Grave, R., Chimini, M., Cattaneo, G., Dalle Grave, A., Ferretti, L., Parolini, S., & Calugi, S. (2024). Intensive cognitive behavioral therapy for adolescents with anorexia nervosa outcomes before, during and after the COVID-19 crisis. Nutrients, 16(10), 1411. https://doi.org/10.3390/nu16101411
Devoe, J. D., Han, A., Anderson, A., Katzman, D. K., Patten, S. B., Soumbasis, A., Flanagan, J., Paslakis, G., Vyver, E., Marcoux, G., & Dimitropoulos, G. (2023). The impact of the COVID-19 pandemic on eating disorders: A systematic review. International Journal of Eating Disorders, 56(1), 5–25. https://doi.org/10.1002/eat.23704
Fairburn, C. G., Cooper, Z., & Shafran, R. (2003). Cognitive behaviour therapy for eating disorders: A "transdiagnostic" theory and treatment. Behaviour Research and Therapy, 41(5), 509–528. https://doi.org/10.1016/S0005-7967(02)00088-8
Gale, R. C., Wu, J., Erhardt, T., Bounthavong, M., Reardon, C. M., Damschroder, L. J., & Midboe, A. M. (2019). Comparison of rapid vs in-depth qualitative analytic methods from a process evaluation of academic detailing in the Veterans Health Administration. Implementation Science, 14(1), 11. https://doi.org/10.1186/s13012-019-0853-y
Graell, M., Morón-Nozaleda, M. G., Camarneiro, R., Villaseñor, Á., Yáñez, S., Muñoz, R., Martínez-Núñez, B., Miguélez-Fernández, C., Muñoz, M., & Faya, M. (2020). Children and adolescents with eating disorders during COVID-19 confinement: Difficulties and future challenges. European Eating Disorders Review, 28(6), 864–870. https://doi.org/10.1002/erv.2763
Guerrini Usubini, A., Cattivelli, R., Varallo, G., Castelnuovo, G., Molinari, E., Giusti, E. M., Pietrabissa, G., Manari, T., Filosa, M., & Franceschini, C. (2021). The relationship between psychological distress during the second wave lockdown of COVID-19 and emotional eating in Italian young adults: The mediating role of emotional dysregulation. Journal of Personalized Medicine, 11, 569. https://doi.org/10.3390/jpm11060569
Leppanen, J., Brown, D., McLinden, H., Williams, S., & Tchanturia, K. (2022). The role of emotion regulation in eating disorders: A network meta-analysis approach. Frontiers in Psychiatry, 13, 793094. https://doi.org/10.3389/fpsyt.2022.793094
Linardon, J., Messer, M., Rodgers, R. F., & Fuller-Tyszkiewicz, M. (2022). A systematic scoping review of research on COVID-19 impacts on eating disorders: A critical appraisal of the evidence and recommendations for the field. International Journal of Eating Disorders, 55(1), 3–38. https://doi.org/10.1002/eat.23640
Micanti, F., Spennato, G., Claudio, R., Amoroso, E., D’Ambrosio, M., Saia, V. M., Barone, A., Tadic, M., Galletta, D., & Vannini, M. (2023). Social media influence on eating disorders since COVID-19 pandemic: A pilot study. European Psychiatry, 66(Suppl. 1), S218. https://doi.org/10.1192/j.eurpsy.2023.509
Monteleone, A. M. (2021). The impact of the COVID-19 pandemic on eating disorders: A paradigm for an emotional post-traumatic stress model of eating disorders. European Neuropsychopharmacology, 51, 84–86. https://doi.org/10.1016/j.euroneuro.2021.05.009
Monteleone, A. M., Cascino, G., Marciello, F., Abbate-Daga, G., Baiano, M., Balestrieri, M., Barone, E., Bertelli, S., Carpiniello, B., Castellini, G., Corrivetti, G., De Giorgi, S., Favaro, A., Gramaglia, C., Marzola, E., Meneguzzo, P., Monaco, F., Oriani, M. G., Pinna, F., Rania, M., Redaelli, C. A., Renna, C., Ricca, V., Salvo, P., Baldissera, E., Segura-Garcia, C., Todisco, P., Volpe, U., Zeppegno, P., & Monteleone, P. (2021). Risk and resilience factors for specific and general psychopathology worsening in people with eating disorders during COVID-19 pandemic: A retrospective Italian multicentre study. Eating and Weight Disorders, 26(8), 2443–2452. https://doi.org/10.1007/s40519-020-01097-x
Monteleone, A. M., Marciello, F., Cascino, G., Abbate-Daga, G., Anselmetti, S., Baiano, M., Balestrieri, M., Barone, E., Bertelli, S., Carpiniello, B., Castellini, G., Corrivetti, G., De Giorgi, S., Favaro, A., Gramaglia, C., Marzola, E., Meneguzzo, P., Monaco, F., Oriani, M. G., Pinna, F., Rania, M., Renna, C., Ricca, V., Salvo, P., Segura-Garcia, C., Scarabel, F., Todisco, P., Volpe, U., Zeppegno, P., & Monteleone, P. (2021). The impact of COVID-19 lockdown and of the following "re-opening" period on specific and general psychopathology in people with eating disorders: The emergent role of internalizing symptoms. Journal of Affective Disorders, 285, 77–83. https://doi.org/10.1016/j.jad.2021.02.037
Onwuegbuzie, A. J., Dickinson, W. B., Leech, N. L., & Zoran, A. G. (2009). A qualitative framework for collecting and analyzing data in focus group research. International Journal of Qualitative Methods, 8(3), 1–21.
Raffagnato, A., Iannattone, S., et al. (2024). The impact of the COVID-19 pandemic on adolescent neuropsychiatric admissions for anorexic eating disorders throughout the 2013–2022 decade. Medical Research Archives, 12(10). https://doi.org/10.18103/mra.v12i10.5833
Schlegl, S., Maier, J., Meule, A., & Voderholzer, U. (2020). Eating disorders in times of the COVID-19 pandemic—Results from an online survey of patients with anorexia nervosa. International Journal of Eating Disorders, 53(11), 1791–1800. https://doi.org/10.1002/eat.23374
Steiger, H., Booij, L., Crescenzi, O., Oliverio, S., Singer, I., Thaler, L., St-Hilaire, A., & Israel, M. (2022). In-person versus virtual therapy in outpatient eating-disorder treatment: A COVID-19 inspired study. International Journal of Eating Disorders, 55(1), 145–150. https://doi.org/10.1002/eat.23655
Termorshuizen, J. D., Watson, H. J., Thornton, L. M., Borg, S., Flatt, R. E., MacDermod, C. M., Harper, L. E., van Furth, E. F., Peat, C. M., & Bulik, C. M. (2020). Early impact of COVID-19 on individuals with self-reported eating disorders: A survey of ~1,000 individuals in the United States and the Netherlands. International Journal of Eating Disorders, 53(11), 1780–1790. https://doi.org/10.1002/eat.23353
Vuillier, L., May, L., Greville-Harris, M., Surman, R., & Moseley, R. L. (2021). The impact of the COVID-19 pandemic on individuals with eating disorders: The role of emotion regulation and exploration of online treatment experiences. Journal of Eating Disorders, 9(1), 10. https://doi.org/10.1186/s40337-020-00362-9
Waller, G., Pugh, M., Mulkens, S., Moore, E., Mountford, V. A., Carter, J., Wicksteed, A., Maharaj, A., Wade, T. D., Wisniewski, L., Farrell, N. R., Raykos, B., Jorgensen, S., Evans, J., Thomas, J. J., Osenk, I., Paddock, C., Bohrer, B., Anderson, K., Turner, H., Hildebrandt, T., Xanidis, N., & Smit, V. (2020). Cognitive-behavioral therapy in the time of coronavirus: Clinician tips for working with eating disorders via telehealth when face-to-face meetings are not possible. International Journal of Eating Disorders, 53(7), 1132–1141. https://doi.org/10.1002/eat.23289
Zipfel, S., Schmidt, U., & Giel, K. E. (2022). The hidden burden of eating disorders during the COVID-19 pandemic. The lancet. Psychiatry, 9(1), 9–11. https://doi.org/10.1016/S2215-0366(21)00435-1