Development of the CBT-E Components Checklist: A tool for measuring therapist self-rated adherence to CBT-E
Suzanne Bailey-Straebler1, 2, PhD, PMH-BC , Zafra Cooper3, DPhil, DipPsych, Riccardo Dalle Grave4, MD, Simona Calugi4, PhD, Rebecca Murphy5, DClinPsych
1 Department of Psychiatry, Weill Cornell Medicine; New York Presbyterian Hospital, White Plains NY, USA, 10605
2 Columbia University School of Nursing, New York, NY, 10032, USA
3 Department of Psychiatry, Yale School of Medicine, New Haven, CT, 06510, USA
4 Department of Eating and Weight Disorders Villa Garda Hospital via Monte Baldo, 89 – 37016 Garda (VR) Italy
5 Department of Psychiatry, University of Oxford, Oxford, OX3 7JX, UK
Abstract
Few tools to encourage therapists to implement evidence based psychological treatments as designed exist. Assessing therapist “competence” (implementing therapeutic procedures well) by evaluating the quality of their treatment sessions is problematic for multiple reasons. Therapist self-rated measures of “adherence” (using the correct therapeutic procedures) may offer a viable alternative. We describe (i) the development of a CBT-E Components Checklist (CBT-E CC) for therapists, as well as (ii) how to use the CBT-E CC and where to access it. The CBT-E CC is an adherence checklist for enhanced cognitive behavior therapy for eating disorders (CBT-E). It is intended as a formative tool for therapists to assess, and improve as needed, their own adherence. Future research on the validity of the checklist to accurately measure adherence is needed.
Keywords
Adherence
Checklist
Self-rated
CBT-E components checklist
Therapist tool
Introduction
The need for scalable adherence tools
Currently, therapists wishing to ensure they are implementing evidence based treatments with fidelity have few options. When available, the traditional method for assessing and encouraging adherence relies on recorded therapy sessions and expert clinician supervision (Herschell et al., 2010; updated, Frank et al., 2020). This method is unattainable for most therapists working in real-world settings as expert supervision is difficult to obtain and costly. Furthermore, even when expert supervision is possible, it often does not involve listening to therapy sessions for a number of reasons. Patients are often uncomfortable with confidential therapy sessions being recorded. Security issues present a further challenge in terms of therapists having both access to secure servers to store the recordings and the ability to send and receive encrypted therapy recordings. And few validated treatment specific therapy competence scales exist.
Recently, self-rated adherence checklists have been examined as an alternative (Serfaty et al., 2020). Checklists are utilized in many fields (e.g., aviation, surgery) to improve the likelihood that all steps of a particular process are completed often with the goal of improving safety (Mahajan, 2011). Specific to psychological therapy, self-rated adherence checklists offer a number of benefits: they are cost effective, easy to use, maintain confidentiality, allow for a greater number of sessions to be rated, and appear to accurately reflect adherence (Serfaty et al., 2020; Caron & Dozier, 2022) with sustained benefit (Caron & Dozier, 2019).
Enhanced Cognitive Behavior Therapy for Eating Disorders CBT-E
CBT-E is short term focused psychological therapy recommended for the treatment of all eating disorders across the age range (NICE, 2017). The treatment is manualized with built-in flexibility. Several adaptations exist, which are tailored to different clinical presentations and age. The treatment typically lasts between 20- 40 sessions depending on whether there is a need to regain weight.
CBT-E focuses on the key mechanisms maintaining the individual’s disorder, including the over-evaluation of eating, shape, and weight – the core psychopathology of most eating disorders. Treatment consists of a series of stages or steps. The treatment for adults is best conceptualized as having four stages, whereas the treatment for adolescents is characterized by three steps (with the stages integrated into these). The beginning of treatment emphasizes understanding the eating disorder, enhancing motivation to change, and specific interventions to normalize eating patterns and regain control. Treatment then focuses on modifying the core psychopathology by decreasing unhelpful behaviors (e.g., body checking, dietary restraint, using eating disorder behaviors to regulate mood), encouraging more helpful ones (e.g., improving body image, developing flexible eating patterns, and building coping skills), and regaining body weight (if indicated). The final Stage of treatment is aimed at maintaining progress and preventing relapse.
Therapists wishing to learn CBT-E can access two detailed treatment “guides” covering adolescents and adults (Fairburn, 2008; Dalle Grave & Calugi, 2020) and a freely available online evidence supported training program (Fairburn et al., 2017). Note that we prefer the term practical “guide” to “manual” as a reminder of the treatment’s flexibility. To assist interested therapists in implementing the treatment as described in the treatment guides and the online training, we created a therapist self-rated adherence checklist: the CBT-E CC.
The CBT-E CC
Development of the CBT-E CC
Core components of CBT-E were identified using the CBT-E treatment guides (Fairburn, 2008; Dalle Grave & Calugi 2020) and a previously developed treatment blueprint (Cooper et al., 2015). An initial pool of items was selected by consensus after discussion among the authors on which to include or discount with a view to obtaining a comprehensive checklist. Treatment experts from the CBT-E training group provided feedback and refinement. There are two main versions of the checklist, one designed to match treatment for adults and one for treatment with adolescents. It does not cover the “broad” modules and is suitable for “focused” elements of CBT-E. Additionally, the CBT-E CC does not provide guidance on how to implement CBT-E or list generic components of treatment (e.g., joint agenda setting, setting and reviewing homework).
Using the CBT-E CC
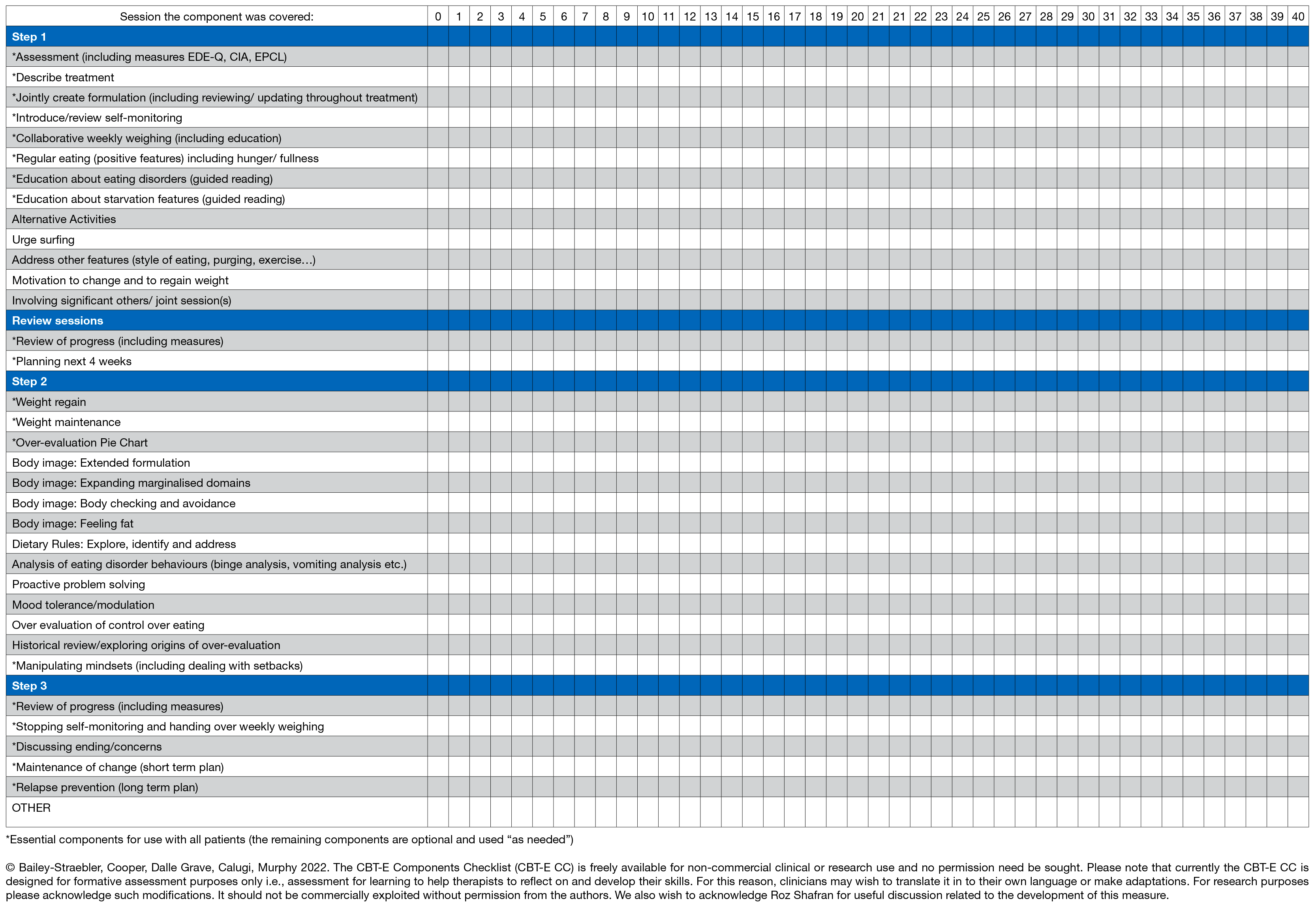
The CBT-E CC is considered part of an implementation package and is best used by therapists who have completed the online training and are familiar with the relevant treatment guide(s). The checklist consists of stages or steps matching the treatment sequence. Therapists should aim to complete the checklist as soon as possible after each treatment session. Checkmarks are placed in boxes corresponding to treatment week indicating which interventions were used in the session. Following the checklist encourages implementation of procedures and can assist in planning future treatment sessions. Prompts to use relevant treatment assessment measures (e.g., Eating Disorders Examination Questionnaire (EDE-Q), Clinical Impairment Assessment (CIA), Eating Problems Checklist (EPCL)) are included. The checklist underlines the importance of flexibility within the treatment by containing both essential and optional treatment interventions.
The CBT-E CC for adults
The CBT-E CC for adults contains 31 items spread across the 4 stages of treatment (Table I). The majority of items are considered essential for treatment and should be included together with a number of optional items. Precise guidance on when to implement these items is not provided to allow for maximum individualization within the treatment. Sessions up to 20 are listed on the checklist with space to add more sessions when needed. Below the essential items are optional items which allow for even further flexibility in delivering the treatment. The version for adults also includes an additional module to use with patients who are underweight, undereating, or are ambivalent about engaging in treatment. It is suggested that when use of this module is necessary sessions should be extended up to approximately 40. At the end of the checklist there is space for the therapist to add any other interventions they would like to track through treatment.
The CBT-E CC for adolescents
The CBT-E CC for adolescents contains 33 items (Table II). The checklist captures the three cumulative sequential steps of treatment. Essential and optional items are listed to encourage flexibility. The adolescent version of the checklist contains 40 sessions by default as the majority of patients in this age group require weight regain. For patients where weight regain is not required, the therapist can remove the extra session boxes. For more detailed session-by-session guidance on treatment procedures used when treating adolescents please see the work of Dalle Grave and Calugi, obtained here: https://www.cbte.co/what-is-cbte/adaptations-for-patient-groups/#adolescents.
The CBT-E CC for adults and adolescents is freely available to therapists providing CBT-E at: https://www.cbte.co/what-is-cbte/adaptations-for-patient-groups/.
Conclusion
Self-rated adherence checklists provide a tool for therapists to efficiently monitor their adherence to treatment protocols. The checklists can be designed with built-in flexibility through the use of essential and optional components. The CBT-E CC is one example. In its current form, the CBT-E CC is a tool for therapists to assess their own levels of adherence. It may also be possible to use it to measure adherence in psychological therapy treatment delivery more widely. Further evidence on the validity of the checklist to be used as a treatment adherence assessment is needed.
Acknowledgements
We would like to acknowledge Professor Roz Shafran for useful discussions which informed the development of the CBT-E CC.
References
Caron, E. B., & Dozier, M. (2022). Self-coding of fidelity as a potential active ingredient of consultation to improve clinicians’ fidelity. Administration and Policy in Mental Health and Mental Health Services Research, 49(2), 237-254.
Caron, E. B., & Dozier, M. (2019). Effects of fidelity-focused consultation on clinicians’ implementation: An exploratory multiple baseline design. Administration and Policy in Mental Health and Mental Health Services Research, 46(4), 445-457.
Cooper, Z., Doll, H., Bailey-Straebler, S., Kluczniok, D., Murphy, R., O’Connor, M. E., & Fairburn, C. G. (2015). The development of an online measure of therapist competence. Behaviour Research and Therapy, 64, 43-48.
Dalle Grave, R., & Calugi, S. (2020). Cognitive behavior therapy for adolescents with eating disorders. Guilford Press: New York.
Fairburn, C. G. (2008). Cognitive behavior therapy and eating disorders. Guilford Press: New York.
Fairburn, C. G., & Cooper, Z. (2011). Therapist competence, therapy quality, and therapist training. Behaviour Research and Therapy, 49(6-7), 373-378.
Fairburn, C. G. (2013). Overcoming binge eating: The proven program to learn why you binge and how you can stop. Guilford press: New York.
Fairburn, C. G., Allen, E., Bailey-Straebler, S., O’Connor, M. E., & Cooper, Z. (2017). Scaling up psychological treatments: a countrywide test of the online training of therapists. Journal of Medical Internet Research, 19(6), e7864.
Frank, H. E., Becker‐Haimes, E. M., & Kendall, P. C. (2020). Therapist training in evidence‐based interventions for mental health: A systematic review of training approaches and outcomes. Clinical Psychology: Science and Practice, 27(3), e12330.
Herschell, A. D., Kolko, D. J., Baumann, B. L., & Davis, A. C. (2010). The role of therapist training in the implementation of psychosocial treatments: A review and critique with recommendations. Clinical Psychology Review, 30(4), 448-466.
Mahajan, R. P. (2011). The WHO surgical checklist. Best Practice & Research Clinical Anaesthesiology, 25(2), 161-168.
National Institute for Health and Care Excellence. (2017). NG69:Eating disorders: Recognition and treatment. https://www.nice.org.uk/guidance/ng69.
Serfaty, M., Shafran, R., Vickerstaff, V., & Aspden, T. (2020). A pragmatic approach to measuring adherence in treatment delivery in psychotherapy. Cognitive Behaviour Therapy, 49(5), 347-360.
Table I. Therapist Self-rated CBT-E Components Checklist for Adults
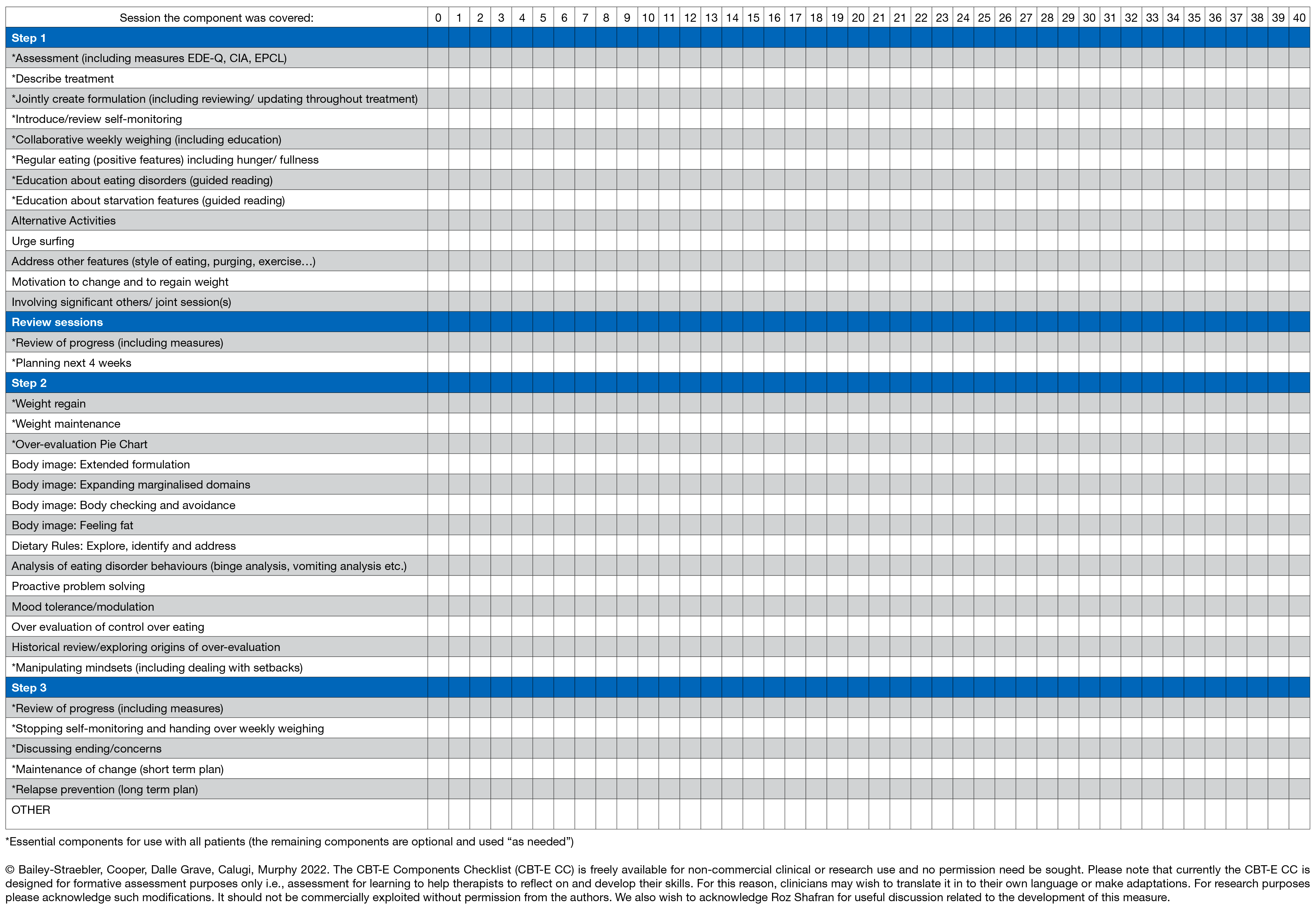
Table II. Therapist Self-rated CBT-E Components Checklist for Adolescents or Patients Who Need to Regain Weight